Obesity and cardiovascular disease
A clinical consensus statement from the National Heart Foundation of Australia

Section 3: Pharmacological and surgical interventions
Pharmacological and surgical interventions play a critical role in the management of overweight and obesity, particularly among those at high cardiovascular risk or with established CVD.186,187
Pharmacotherapy is indicated for obesity management, in conjunction with behaviour modifications, when adequate weight-related health improvements cannot be attained through behaviour modifications alone. Weight loss of approximately 5–10% of total body weight is generally required to attain these weight-related health improvements.188,189 Pharmacotherapy should complement, not replace, behaviour modifications.106,190,191
Incretin-based medicines (including GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists) have changed the landscape of obesity management. High quality trials have demonstrated incretin-based medicines improve cardiometabolic risk factors and, in some cohorts, reduce the risk of major adverse cardiovascular events.11,12 Across trials, they have consistently led to substantial weight loss, achieving reductions exceeding 10% of baseline body weight.11,190,192,193 To note, real world observational data suggest that average weight loss is lower than that seen in randomised controlled trials due to a combination of lower achieved dosages, treatment interruptions and high discontinuation rates (up to 20–50% within the first year).194,195
General practitioners are well-placed to support people in commencing obesity management medications and to support ongoing care. Weight regain is common after ceasing these agents, therefore they are likely to be needed long term.196
For people who are unable to attain weight-related health improvements with behaviour modifications and pharmacotherapy, or unable to sustain weight loss after treatment discontinuation, referral to specialised care is generally required. This may include consideration of metabolic bariatric surgery to achieve weight goals and improve cardiovascular health.
Multiple systematic reviews and meta-analyses, of predominantly cohort studies, have shown that metabolic bariatric surgery is consistently associated with reduced cardiovascular morbidity and mortality among individuals with obesity (predominantly in people at high risk of CVD with some lower quality evidence demonstrating benefit in people with established disease).187,197-202
Procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass not only achieve sustained weight loss, but can also induce remission of type 2 diabetes, lower blood pressure, improve lipid profiles, and may reduce the risk of heart failure exacerbations.203-206 Metabolic bariatric surgery has also been associated with short term improvements in mental health, depressive symptoms and quality of life, but longer‑term mental health outcomes are heterogeneous.207-209
Access and cost remain significant barriers for obesity management medications and metabolic bariatric surgery. There are currently no Therapeutic Goods Administration-approved incretin-based medicines available on the Pharmaceutical Benefits Scheme (PBS) for obesity management (Table 7). This means the cost remains prohibitive for many people.210 At the time of writing, the Pharmaceutical Benefits Advisory Committee has made a positive recommendation for semaglutide in a subgroup of people with obesity and established CVD.211
Similarly, metabolic bariatric surgery has limited availability in the vast majority of Australian public hospitals, with more than 90% of procedures taking place in the private sector.212 Financial barriers are likely to compound inequities given the disproportionate burden of obesity and CVD in priority populations who may have limited access to private medical and surgical care.210 With a growing prevalence of obesity and overweight in Australia, expediting mechanisms to improve access to multidisciplinary obesity care is critical.
Pharmacotherapy
Recommendations |
Strength of advice |
|---|---|
|
Obesity management medications are indicated, in conjunction with behaviour modifications, when adequate weight-related health improvements cannot be attained through behaviour modifications alone. |
Strong advice |
|
In adults living with established atherosclerotic CVD and BMI ≥ 27 kg/m2, consider prescribing a GLP-1 receptor agonist with proven CVD benefit (semaglutide) to reduce the risk of major adverse cardiovascular events. |
Moderate advice |
|
In adults living with heart failure with preserved ejection fraction (HFpEF) and obesityα, consider semaglutide or tirzepatide to improve symptoms and functional capacity. |
Moderate advice |
|
In adults living with type 2 diabetes and overweight or obesity, with or without CVD, consider a GLP-1 or GIP/GLP-1 receptor agonist with proven CVD benefit (semaglutide, liraglutide or tirzepatide) to reduce the risk of major adverse cardiovascular events. |
Strong advice |
|
αDefined in trials as BMI ≥ 30 kg/m2 and ejection fraction ≥ 50% (SUMMIT, tirzepatide) or ejection fraction ≥ 45% (STEP-HFpEF, semaglutide). While these medications have demonstrated benefit for heart failure symptoms and quality of life, they are not yet approved by the Therapeutic Goods Administration for management of this condition. |
|
General information
Obesity management medications approved for use in Australia by the Therapeutic Goods Administration (TGA) are listed in Table 8.
The injectable GLP-1 receptor agonists (e.g. semaglutide, liraglutide) and GIP/GLP-1 receptor agonists (tirzepatide) promote weight loss via several different mechanisms of action (Figure 5). Cardiovascular outcome trials of these agents have also demonstrated improvement in cardiometabolic markers including blood pressure and lipid profiles.190,213
GLP-1 receptor agonists act by binding to and amplifying activation of the GLP-1 receptor, resulting in enhanced post-prandial insulin secretion, glucagon release inhibition, delayed gastric emptying and appetite suppression.214
The cardioprotective effects of semaglutide may be independent of its impact on weight, suggesting additional underlying mechanisms, including anti-inflammatory effects such as reductions in systemic inflammatory markers, which may contribute to cardiovascular benefit.215,216
The GIP/GLP-1 receptor agonists have an additional agonism effect at the GIP receptor, resulting in increased insulin secretion in a glucose dependent manner and combined effects on appetite regulation and weight loss.217,218
Table 8: Therapeutic Goods Administration-approved obesity management medications, their indications and relevant PBS criteria
Medication name |
TGA indications |
PBS criteria (for obesity management) |
|---|---|---|
Incretin-based agents |
||
| Semaglutide | Management of weight in adults with a BMI ≥ 30 kg/m² or ≥ 27 kg/m² in the presence of one or more weight-related complications. | Not included on PBS* |
| Tirzepatide | Management of weight in adults with a BMI ≥ 30 kg/m² or ≥ 27 kg/m² in the presence of one or more weight-related complications. | Not included on PBS |
| Liraglutide | Management of weight in adults with a BMI ≥ 30 kg/m² or ≥ 27 kg/m² in the presence of one or more weight-related complications. | Not included on PBS |
Oral agents |
||
| Orlistat | Management of weight in adults with a BMI ≥ 30 kg/m² or ≥ 27 kg/m² in the presence of one or more weight-related complications. | Included on Repatriation Pharmaceutical Benefits Scheme, for individuals with BMI ≥ 35 kg/m² with no known co-morbidities or BMI ≥ 30 kg/m² with at least one co-morbidity. |
| Naltrexone/bupropion | Management of weight in adults with a BMI ≥ 30 kg/m² or ≥ 27 kg/m² in the presence of one or more weight-related complications. | Not included on PBS |
| Phentermine | Management of weight in adults with a BMI ≥ 25 kg/m². | Not included on PBS |
* At the time of writing, the Pharmaceutical Benefits Advisory Committee has made a positive recommendation for semaglutide in a subgroup of people with obesity and established CVD.

Figure 5: Mechanisms of action of GLP-1 receptor agonists and GIP/GLP-1 receptor agonists.190,219-222
*Further research is required to fully understand the cardioprotective mechanisms of these agents.
Abbreviations: GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1; HbA1c, haemoglobin A1c.
Compared with injectable pharmacotherapies, the oral agents orlistat, naltrexone/bupropion and phentermine are less effective for weight loss and lack CVD outcome data (Table 9).
For phentermine, there are several CVD-related contraindications (e.g. valvular disease, arrhythmias and advanced arteriosclerosis) and precautions (e.g. mild hypertension). Similarly, naltrexone/bupropion is contraindicated in people with uncontrolled hypertension and is cautioned in people with controlled hypertension.223-225 Refer to individual agent product information for more detail.
Table 9: Pharmacotherapies for obesity management219,223,224,226-243


Figure 6:Efficacy of weight management interventions for weight loss.*83,228,236-238,245-249
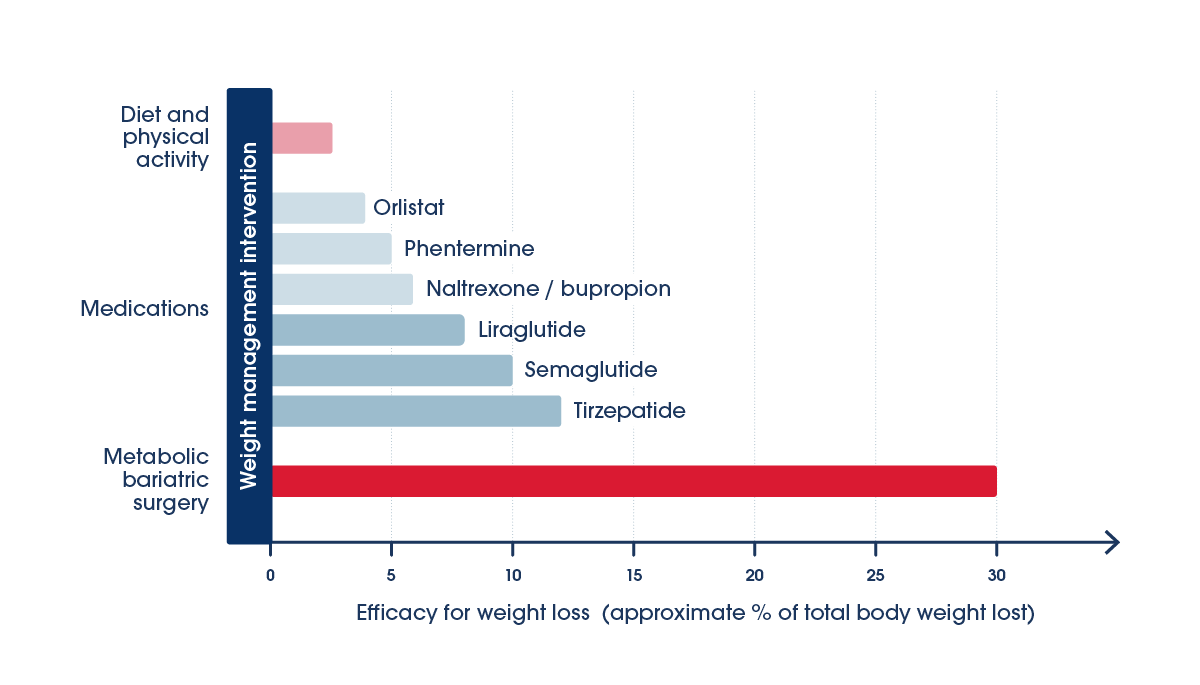
*To note, the efficacy for weight loss percentages represents findings from several studies of varying cohorts and study quality. They do not represent head-to-head comparison studies and are intended to provide a general indication of comparative efficacy. Figures for semaglutide and tirzepatide have been derived from published cardiovascular outcome trials. In the case of liraglutide, the SCALE trial was used as the reference for percentage total body weight lost, in preference to the LEADER cardiovascular outcome trial. The latter used approximately half the maintenance dose of liraglutide that is indicated for weight management. For each intervention, the bar represents the upper end of the range for approximate percentage of total body weight loss.
Practice points
Initiation and titration
- Pharmacotherapy may be considered when weight-related health improvements, such as improvements in lipids, blood glucose levels, blood pressure and metabolic dysfunction-associated steatotic liver disease, have not been attained with behaviour modifications alone, or the weight loss required is higher than what can be achieved through behaviour modifications.
- Pharmacotherapy for obesity management should be initiated as part of a comprehensive management plan, which includes the continuation of behaviour modifications (nutrition and physical activity).
- In certain cases, especially among individuals with a higher BMI and existing complications, initiation of pharmacotherapy may be warranted as a first-line intervention along with behaviour modifications. Shared decision-making is critical at that stage, factoring in the person’s preferences and values. The high cost of obesity management medications, particularly incretin-based agents, means they remain inaccessible for many people.
- The starting dose of semaglutide is 0.25 mg subcutaneous once weekly, which can be increased incrementally every four weeks to a maintenance dose of 2.4 mg:250
weeks 1–4: 0.25 mg
weeks 5–8: 0.5 mg
weeks 9–12: 1 mg
weeks 13–16: 1.7 mg
maintenance dose: 2.4 mg.
Slow initiation helps to minimise gastrointestinal side effects.
To note, Wegovy (semaglutide) is a higher dose semaglutide formulation which has been approved by the TGA for chronic weight management at a maximum dose of 2.4 mg weekly. Ozempic is only TGA-approved for type 2 diabetes. Oral formulations of semaglutide exist (one is TGA-approved for diabetes) but are not commercially available in Australia at the time of writing. A higher dose injectable semaglutide formulation (7.2 mg) is currently pending TGA approval.251
- The starting dose of tirzepatide is 2.5 mg subcutaneous once weekly. After four weeks, the dose can be increased to 5 mg weekly. Dose can be further increased by 2.5 mg every four weeks to a maximum dose of 15 mg once weekly as required.252
- The starting dose of liraglutide is 0.6 mg subcutaneous once daily. Doses should be increased in 0.6 mg increments at intervals of at least one week to a maintenance dose of 3 mg daily.219,234
- Oral agents (e.g. orlistat, naltrexone/bupropion and phentermine) have a limited role in the management of overweight/obesity in people with or at high risk of CVD due to their minimal impact on weight, unknown CVD benefits and poor tolerability.
- After commencement of pharmacotherapy, regularl assessment of weight, cardiometabolic risk factors and treatment tolerability should be undertaken. The dose of pharmacotherapy should be adjusted if required to achieve health targets (increasing or decreasing the dose). Monitor for nutritional adequacy if clinical concerns such as poor diet quality, disordered eating behaviour or very rapid weight loss occur (typically > 1.5–2 kg per week). See section on ‘Dietary advice for people on incretin-based medications’. Engage multidisciplinary team, including pharmacists and allied healthcare professionals, to support adherence.
- Advise people that ongoing pharmacotherapy, in conjunction with behaviour modifications, is likely to be needed to maintain a healthy weight and effectively manage CVD risk in the long term. Weight regain is common after cessation of pharmacotherapy. Some studies show up to 60% of weight lost during treatment is regained one-year post cessation,196 and cardiometabolic risk factor improvements may be reversed (e.g. HbA1c, cholesterol and blood pressure).253
Side effects
- Advise people that the most common side effects of incretin-based obesity management medications are gastrointestinal and can include nausea, diarrhoea, constipation and vomiting. These side effects have been reported in approximately 20–40% of people and are most common during dose initiation and escalation.250,252 In most people, these side effects can be mitigated by commencing at a lower dose and titrating the dose gradually over weeks.
- People should be advised that having smaller, more frequent meals and avoiding fatty foods can alleviate nausea and vomiting side effects during treatment initiation.254 Adequate fluid and fibre intake can also help alleviate the side effect of constipation.254
- The use of GLP-1 receptor agonists has been associated with rarer side effects including an increased risk of acute pancreatitis, gastroparesis and intestinal obstruction although incidence is rare (<0.1%).219 Inform people about the symptoms of pancreatitis and when to seek medical attention.250 If pancreatitis occurs, the GLP-1 receptor agonist should not be restarted. Similarly, exercise caution when commencing these medications in people with a history of acute pancreatitis.
- A newly identified safety signal, based on a small number of case reports, indicates a possible association between GLP-1 receptor agonists (including tirzepatide) and suicidal ideation.255,256 Whilst international regulators (e.g. US Food and Drug Administration) have now removed such warnings, the Therapeutic Goods Administration has updated product safety warnings and advised healthcare professionals to monitor people for changes in mood, behaviour or emerging suicidal thoughts or behaviours.
- Case reports have linked GLP-1 receptor agonists and GLP-1/GIP receptor agonists to an increased potential risk of regurgitation and pulmonary aspiration during anaesthesia due to delayed gastric emptying.257 Preprocedural clinical consensus advice should be followed (see Resources and further reading).
- Advise people that most over-the-counter and online weight loss products, including complementary and herbal supplements, have limited or no evidence for their safety and efficacy. Counterfeit medications disguised as weight loss products are not uncommon. These agents are illegal and can contain harmful, undisclosed ingredients, including sibutramine which has been shown to increase the risk of heart attack and stroke.258
Lean muscle mass loss
- Sarcopenia (loss of muscle strength, mass and function) can be exacerbated by chronic comorbidities, including CVD, and is associated with faster disease progression and higher mortality in these groups.259
- Maintenance of lean mass is important during weight loss because muscle mass facilitates a higher metabolic rate and makes it easier to lose and maintain body weight after a weight loss intervention.
- While dietary weight loss strategies typically cause some loss of lean muscle, GLP-1 and GIP/GLP-1 receptor agonists are associated with significant loss of lean mass ranging from 15–45% of total weight loss,260 varying by agent.
- Strategies to mitigate lean muscle loss while on treatment include optimising dietary protein, recognising that GLP-1 and GIP/GLP-1 receptor agonists may suppress appetite and substantially reduce overall energy intake, increasing the risk of inadequate protein consumption.260-262
- Regular resistance exercise training can help preserve lean muscle mass during weight loss and should be performed on two or more days per week, where clinically appropriate.159
Dietary advice for people on incretin-based medications
- Incretin-based medications increase the risk of muscle loss, sarcopenic obesity and nutrient deficiencies.263 Prescribers of obesity management medications should consider concurrent referral to an Accredited Practising Dietitian to optimise outcomes.263
- People on incretin-based medications should prioritise adequate protein intake (1.2–1.60 g/kg of body weight per day, or an absolute target of 80–120 g/day where appropriate),254 combined with structured resistance exercise, to support preservation of lean mass during weight loss. Increased protein intake alone is unlikely to preserve muscle mass in the absence of resistance training.
- Supplementation may assist in meeting protein and micronutrient requirements when dietary intake is insufficient.263
- Reduced appetite with GLP‑1 receptor agonists may result in unintentional intermittent fasting. Individuals should be encouraged to consume meals at regular intervals, as prolonged fasting without adequate protein intake or dietary variety may increase the risk of nutritional inadequacy.254
- More aggressive caloric restriction strategies including LEDs and VLEDs are generally not appropriate in combination with incretin-based medications unless under close specialist supervision with monitoring of body composition and nutritional status.
Considerations in people with type 2 diabetes
- In adults living with type 2 diabetes and overweight or obesity, consider prescription of glucose-lowering agents with dual weight management and cardiovascular benefits to reduce the risk of major adverse cardiovascular events.
- GLP-1 receptor agonists with demonstrated cardiovascular benefit in people with type 2 diabetes include liraglutide,227 semaglutide,229 and dulaglutide.264
- Tirzepatide, a GIP/GLP-1 receptor agonist, has also demonstrated cardiovascular benefit in people with type 2 diabetes.245
- At the time of writing, semaglutide and dulaglutide can only be prescribed on the PBS for type 2 diabetes specifically, not obesity management.
- SGLT-2 inhibitors (such as empagliflozin and dapagliflozin) are also indicated for the treatment of type 2 diabetes and have been shown to have modest weight-lowering effects in this population.265 These drugs offer significant cardiovascular and renal benefits.266
- Healthcare professionals should be aware of potential drug interactions with the use of GLP-1 receptor agonists and GIP/GLP-1 receptor agonists in combination with other glucose-lowering agents (e.g. sulfonylureas, insulin) due to an increased risk of hypoglycaemia.250,252 Monitor and consider titrating the dose of sulfonylurea or insulin when commencing a GLP-1 receptor agonist or GIP/GLP-1 receptor agonist.267
- In people with type 2 diabetes, assess for retinopathy during GLP-1 receptor agonist initiation and titration, due to the increased risk of retinopathy associated with a rapid reduction in glycosylated haemoglobin (HbA1c).268
- Emerging safety signals suggest a possible rare association between GLP-1 receptor agonists (particularly semaglutide) and GIP/GLP-1 receptor agonists, and non-arteritic anterior ischemic optic neuropathy in people with type 2 diabetes, however further research is warranted.269-271
Considerations in older people
- Evidence for the safety and efficacy of obesity management medications in older people is limited. Healthcare professionals should consider the increased risk of sarcopenia and nutrient deficiencies when prescribing these medications and reinforce appropriate nutrition and resistance training.263,272
Considerations in women
- Women of reproductive age taking a GLP-1 receptor agonist or tirzepatide should be advised to use contraception concurrently due to potential safety concerns associated with taking these pharmacotherapies in pregnancy (as shown in animal studies).273,274 Semaglutide and tirzepatide are both classified as pregnancy category D medications.250,252
- Tirzepatide and GLP-1 receptor agonists may decrease absorption of oral contraceptives due to delayed gastric emptying, however the evidence is inconsistent.275 As a precaution to avoid unplanned pregnancy, current product information for tirzepatide includes advice that women should switch to a non-oral contraceptive or add a barrier method of contraception for four weeks after initiation, and for four weeks after each dose escalation.276 This advice has not been extended to GLP-1 receptor agonists (liraglutide and semaglutide) at the time of writing.
Considerations in people with heart failure
- When initiating and escalating semaglutide or tirzepatide in people with obesity and heart failure with preserved ejection fraction (HFpEF), monitor kidney function and electrolytes and adjust other medications (e.g. diuretics, antihypertensives, glucose-lowering agents) if required, particularly if the person is experiencing gastrointestinal side effects.277
- Semaglutide and tirzepatide have been shown to improve quality of life and functional capacity in people with HFpEF and BMI ≥ 30 kg/m2, but insufficient evidence exists to conclude cardiovascular outcome benefits.278,279
- There is a lack of high-quality trial data evaluating the cardiovascular impact of GLP-1 receptor agonists in people with heart failure with reduced ejection fraction.
- SGLT-2 inhibitors are also indicated for the management of both reduced and preserved ejection fraction heart failure and may have modest weight-lowering effects in these populations.280 These medications include empagliflozin and dapagliflozin, which are included on the PBS for the indication of chronic heart failure.
Considerations in people with other comorbidities
- Tirzepatide is also indicated for the treatment of moderate-to-severe obstructive sleep apnoea in adults with obesity.252
- GLP-1 receptor agonists have emerged as an important treatment option for diabetic kidney disease in the context of type 2 diabetes, with semaglutide showing reduced risk of clinically important kidney outcomes and death from cardiovascular causes in people with type 2 diabetes and chronic kidney disease.281
- Incretin-based therapies are emerging as a treatment for metabolic dysfunction-associated liver disease (formerly non-alcoholic fatty liver disease), with evidence suggesting benefits in liver histology and a reduction in liver fat.282,283 The Therapeutic Goods Administration has recently provisionally approved semaglutide for the treatment of non-cirrhotic metabolic dysfunction-associated steatohepatitis (MASH) in adults with moderate to advanced liver fibrosis.231,284
Summary of the evidence
- Evidence for the use of incretin-based therapies in a CVD primary prevention cohort largely draws from trials involving people with type 2 diabetes. The LEADER, SUSTAIN-6, and REWIND trials collectively demonstrate the cardiovascular outcome benefits of GLP-1 receptor agonists in people with type 2 diabetes and at high CVD risk.
- LEADER (9,340 participants, median 3.8 years) showed liraglutide reduced major adverse cardiovascular events compared with placebo (HR 0.87; 95% CI 0.78–0.97).227
- SUSTAIN-6 (3,297 participants, median two years) found semaglutide provided an even greater relative risk reduction compared with placebo (HR 0.74; 95% CI 0.58–0.95).229
- REWIND (around 9,900 participants, approximately one third with established CVD, median 5.4 years) demonstrated dulaglutide lowered major adverse cardiovascular event risk compared with placebo (HR 0.88; 95% CI 0.79–0.99).264
- The cardiovascular outcome trial for tirzepatide (SURPASS-CVOT) has demonstrated cardiovascular benefit in people with type 2 diabetes and atherosclerotic CVD.229,245,285 In SUPRASS-CVOT, tirzepatide was found to be non-inferior to dulaglutide (HR 0.92; 95% CI 0.83-1.01).245 At the time of writing, the SURMOUNT-MMO trial is currently underway to investigate the cardiovascular outcomes of tirzepatide in people with overweight/obesity without type 2 diabetes.286
- The landmark SELECT trial has demonstrated the cardiovascular benefits of the GLP-1 receptor agonist, semaglutide (2.4 mg subcutaneous once weekly), in people established atherosclerotic CVD and with a BMI ≥ 27 kg/m2 (without type 2 diabetes). In this double-blind, placebo-controlled randomised clinical trial of 17,604 adults, semaglutide reduced the incidence of cardiovascular death, myocardial infarction and stroke (HR 0.80; 95% CI 0.72–0.90).228
- There is growing evidence to support the role of GLP-1 receptor agonists and GIP/GLP-1 receptor agonists in improving heart failure-related symptoms and quality of life in people with HFpEF in the setting of obesity,278,279 and in concurrent obesity and type 2 diabetes.287 In the SUMMIT trial, tirzepatide showed a significant reduction in heart failure events in people with HFpEF but results should be interpreted with caution due to small event numbers.279
- Emerging unpublished observational data suggest that GLP-1 receptor agonists may also play a secondary prevention role in people with atrial fibrillation, obesity and type 2 diabetes, although further research is underway.288
Resources and further reading
- Australian Register of Therapeutic Goods Product Information
- Pharmaceutical Benefits Scheme
- Australian Diabetes Society. Clinical practice recommendations: Periprocedural use of GLP-1 RAs and GLP-1/GIP RAs
Emerging pharmacotherapies
Several novel obesity management medications and formulations are currently being investigated in clinical trials. Some selected new therapies on the horizon are discussed below.
- Retatrutide, a triple agonist against GLP-1, GIP and glucagon receptors, has demonstrated significant weight loss (up to a 24% reduction in body weight at the highest dose) and metabolic benefits in people with obesity, both with and without type 2 diabetes in phase 2 clinical trials.289,290
- Survodutide is a novel dual glucagon receptor and GLP-1 receptor agonist.291 In phase 2 trials, it conferred significant weight loss (up to 19% of total body weight) in people with obesity without type 2 diabetes.292 Phase 3 clinical trials are currently underway in both people with and without type 2 diabetes, in addition to a cardiovascular outcomes trial.293
- Oral semaglutide (25 mg) daily achieved 11.4% reduction in body weight compared with placebo (95% CI -13.9-9.0) in people with overweight and obesity.294 While not a head-to-head study, this is comparable to observed body weight reduction achieved with subcutaneous semaglutide 2.4 mg weekly. Trials have demonstrated that oral semaglutide reduces the risk of major adverse cardiovascular events (HR 0.86; 95% CI 0.77 to 0.96) in people with type 2 diabetes and established CVD and/or chronic kidney disease, without an increase in risk of serious adverse events.295
- A novel oral GLP-1 receptor agonist – orforglipron– has shown significant glycaemic and weight loss benefits in people with and without type 2 diabetes.296-298
- CagriSema, a combination of cagrilinitide and semaglutide, is a dual GLP-1 receptor agonist and long-acting amylin analogue. The REDEFINE trials have shown that CagriSema confers clinically significant weight loss (approximately 20% of total body weight) compared with placebo, in both people with and without type 2 diabetes.299,300
- Phase 2 trials of once weekly administration of the amylin receptor agonist, eloralintide, in adults with overweight or obesity and without type 2 diabetes have demonstrated significant weight loss, with a mean decrease in body weight ranging from 9–16%, compared with 0.4% in the placebo group.301 Combination therapy of amylin and semaglutide has also shown promise in weight management, with over 40% of trial participants achieving a decrease in body weight of ≥ 25%.302
- Monthly injectable agents have shown promise in the treatment of obesity in adults with and without type 2 diabetes. Maridebart cafraglutide (MariTide) is a combined GLP-1 receptor agonist and GIP receptor antagonist. Results from a phase 2 clinical trial suggest this pharmacotherapy produces clinically significant weight loss compared with placebo.303
Several other pharmacotherapies are used off label, including lisdexamfetamine and a combination of phentermine and topiramate, but none are Therapeutic Goods Administration-approved for weight loss in Australia.
Surgical interventions
Recommendations |
Strength of advice |
|---|---|
|
In adults living with overweight or obesity and CVD or at high risk of CVD who have not attained adequate weight-related health improvements through behaviour modifications and pharmacological interventions, consider referral to multidisciplinary specialised obesity services. |
Moderate advice |
|
In adults with CVD or at high risk of CVD with BMI ≥ 40 kg/m2 or, BMI ≥ 35 kg/m2 with at least one weight-related comorbid condition¥, refer for consideration of metabolic bariatric surgery to reduce the risk of major adverse cardiovascular events. |
Moderate advice |
|
In adults with CVD or at high risk of CVD who have undergone metabolic bariatric surgery, offer lifelong multidisciplinary follow‑up care to support long term health. |
May be appropriate |
|
¥Weight-related comorbid conditions include hypertension, dyslipidaemia, obstructive sleep apnoea, cardiovascular disease, prediabetes or type 2 diabetes. |
|
General information
Differences in eligibility criteria for metabolic bariatric surgery differ locally and internationally. The BMI criteria presented in this statement align with the current Medicare Benefits Schedule criteria for metabolic bariatric surgery.304 These criteria also reflect the absence of randomised controlled trial evidence of improved cardiovascular outcomes in people with a lower BMI (30–34.9 kg/m2) undergoing metabolic bariatric surgery. While surgery is highly effective for weight loss, evidence of cardiovascular benefit in this cohort is largely based on observational studies and small randomised controlled trials demonstrating improvement in surrogate cardiovascular measures only.305-307 The first randomised controlled trial investigating the impact of metabolic bariatric surgery in improving cardiovascular outcomes is currently underway.304,308
Practice points
Eligibility and pre-surgical assessment
- Multidisciplinary specialised obesity services provide medically led, multidisciplinary care that incorporates nutrition and physical activity interventions, psychological therapies, pharmacological treatment, and access to metabolic bariatric surgery where clinically appropriate and feasible. Referral to multidisciplinary specialised obesity services from primary care should be considered:
- when sustained weight-related health improvements (such as improvements in lipids, blood glucose, blood pressure or metabolic dysfunction-associated steatotic liver disease) have not been attained via behaviour modifications and pharmacotherapy, or
- in complex clinical scenarios, or
- in individuals who meet the Medicare Benefits Schedule criteria for metabolic bariatric surgery.
- The most common types of metabolic bariatric surgery performed in Australia are sleeve gastrectomy, Roux-en-Y gastric bypass and single anastomosis gastric bypass (Table 10).
- Discuss the potential benefits and risks of metabolic bariatric surgery with people, including the requirement for lifelong monitoring and multidisciplinary follow up. Referral to specialist care for consideration of surgery should be undertaken as part of a shared decision-making process.
- Comprehensive pre-surgical assessment by a multidisciplinary specialist team is important. This should include assessment of cardiometabolic risk, screening for mental health conditions, eating disorders and nutritional deficiencies, and an assessment of psychological and overall fitness for surgery. Ensure input from surgeons, endocrinologists, cardiologists, psychologists and dietitians as appropriate.
Post-surgical monitoring and follow up
- People who have undergone metabolic bariatric surgery should be monitored following surgery for:
- micronutrient deficiencies
- protein-energy malnutrition
- mental health conditions (e.g. depression, addictive disorders, eating disorders)
- weight regain or excessive weight loss
- gastrointestinal side effects or complications, including gall stones
- medication side effects due to altered pharmacokinetics
- bone health.
Refer to Table 11 for further detail.
- Post-surgery care should include an integrated care plan such as support for nutrition, physical activity, behavioural strategies, and psychological wellbeing.
- Monitor people for dumping syndrome following bariatric surgery, which can occur when a person consumes high sugar or high carbohydrate foods and drinks. These types of foods/drinks pass too quickly from the stomach into the small intestine, causing gastrointestinal symptoms (e.g. nausea, vomiting, bloating, diarrhoea) and hypoglycaemia.
- Some people may require obesity management medication post-surgery to support weight maintenance. Healthcare professionals should assess the need to commence pharmacotherapy (or continue pharmacotherapy if commenced prior to surgery), monitor for side effects, and titrate the dose accordingly. Involve pharmacists as appropriate.
- A small subset of people experience increased risk of alcohol or other substance use disorders post-operatively, particularly following gastric bypass procedures.309 Population data suggest new-onset substance use disorder occurs in a small minority.310 Risk should be addressed through pre-operative screening and longitudinal monitoring, particularly in individuals with prior substance use and mental health disorders.
Dietary advice post-bariatric surgery
- Advise consumption of small, frequent meals (typically 4–6 per day) eaten at regular intervals to improve tolerance, optimise nutrient intake, and reduce the risk of dumping syndrome and post-prandial hypoglycaemia.311
- Protein-rich foods should be included with each meal and snack to support lean mass preservation, enhance satiety and to moderate post‑prandial glycaemic responses.312
- Foods and drinks high in added sugars or refined carbohydrates should be minimised, as they can precipitate early dumping symptoms and late post-prandial (reactive) hypoglycaemia following bariatric procedures.313,314
- People are advised to avoid drinking with meals and to separate fluids from solid food intake (commonly by ~30 minutes) to slow gastric emptying, improve nutrient absorption, and reduce dumping related‑symptoms.311
- Encourage slow eating, thorough chewing, and mindful portion control to improve gastrointestinal tolerance and support recognition of early satiety.315
- Soluble fibre and modest amounts of dietary fat may help slow nutrient absorption and reduce glycaemic variability, though tolerance should be individualised and guided by dietitian review.313
- Long‑term dietary management following bariatric surgery should be supported by regular dietitian review to address nutritional adequacy, symptom management, and evolving risks such as dumping syndrome, hypoglycaemia or micronutrient deficiencies.
Accessibility
- Accessibility of metabolic bariatric surgery services remains a significant barrier in Australia, with only a very small minority of Australian public hospitals offering these services.316 Around 90% of metabolic bariatric surgeries, which are generally high cost, take place in the private sector.316
- Uptake of metabolic bariatric surgery is impacted by both financial and geographical barriers including affordability of private health insurance with surgical cover, limited availability of services in rural and remote areas and low referral rates.317
Table 10. Comparison of selected metabolic bariatric procedures in Australia.318-327
Table 10 |
Sleeve gastrectomy |
Roux-en-Y gastric bypass (RYGB) |
Single anastomosis (one anastomosis) gastric bypass |
Single anastomosis duodenal-ileal interposition |
|---|---|---|---|---|
|
Procedure details |
Removes ~75–80% of the stomach, leaving a narrow sleeve |
Creates a small gastric pouch and reroutes small intestine |
Similar to RYGB but with one intestinal anastomosis |
Combines a sleeve gastrectomy with a single anastomosis connecting the duodenum to the distal ileum |
|
Proportion of bariatric surgeries |
~77% |
~9% |
~13% |
<1% |
|
Mean % weight loss |
~25–30% at 1–2 years |
~25–30% at 1–2 years |
~30–35% at 1–2 years |
~30–40% at 1–2 years |
|
Nutritional concerns |
- Nutritional deficiencies |
- Greater frequency of nutritional deficiencies |
- Even greater frequency of nutritional deficiencies |
- Higher risk of protein-energy malnutrition |
|
Advantages |
- Shorter operative time |
- Excellent metabolic benefits |
- Greater weight loss |
- Even greater weight loss and more durable |
|
Disadvantages and risks |
- Irreversible |
- Risk of dumping syndrome |
- Risk of bile reflux |
- Marginal ulcers (rare) |
Abbreviations: GORD, gastroesophageal reflux disease.
Table 11: Common issues following metabolic bariatric surgery and actions primary healthcare professionals can consider.312,328-340
| Post-surgical issue | Risk | Primary healthcare professional actions to consider |
|---|---|---|
| Nutritional deficiencies | Common nutritional deficiencies include iron, folate, calcium (check PTH), vitamins A, B1, B6, B12, D |
- Conduct regular blood tests (every six months initially post-surgery, then six monthly or annually) - Refer to an Accredited Practising Dietitian, or another appropriately qualified healthcare professional if not available - Prescribe lifelong multivitamin and mineral supplements (and procedure-specific additional supplements) |
| Weight regain | Weight regain is to be expected and should be managed early as required |
- Monitor weight regularly - Support people to maintain ongoing nutrition and physical activity - Consider commencing pharmacotherapy to maintain weight, where clinically appropriate |
| Gastrointestinal symptoms |
- Reflux - Change in stool frequency |
- Prescribe a regular proton pump inhibitor in early post-operative phase - Dietary interventions to assist with stool frequency - Consider surveillance gastroscopy for Barrett’s oesophagus at one year, then every 2–3 years (particularly important for people with sleeve gastrectomy or single anastomosis gastric bypass) |
| Mental health | Potential risk of relapse of psychiatric disorders and/or the emergence of new psychiatric disorders perioperatively, including mood, anxiety, eating and/or substance use disorders | - Where relevant, undertake screening for mental health conditions, substance abuse and other addictive or compulsive behaviours with referral pathways (Refer to Appendix 4: Mental health and eating disorder validated assessment tools for a list of validated mental health screening tools) |
| Medication titration | Altered pharmacokinetics of some medications (e.g. oral contraceptive pill, psychiatric medications) may necessitate dose or formulation changes, or alternative treatment options |
- Monitor and titrate dose of medications as required - Seek blood levels of psychiatric medications where relevant - Seek pharmacy input as required |
| Bone health | Potential loss of bone mineral density (osteopenia/osteoporosis) due to nutrient malabsorption (calcium, vitamin D, zinc, copper), menopause, rapid weight loss and mechanical unloading. This may also lead to higher fracture risk |
- Measure serum PTH, calcium phosphorus, vitamin D, 24-hour urine calcium levels - Lifelong calcium supplementation generally recommended - Vitamin D supplementation should be individualised and guided by serum 25-OH vitamin D levels; interpret in conjunction with corrected calcium and PTH concentrations - Consider DEXA scanning in higher risk people |
| Pregnancy and contraception |
Oral contraception may not be as reliable post-surgery Increased risk of unplanned pregnancy resulting from weight loss (due to improved fertility) |
- Consider alternative contraceptive options that do not rely on absorption (i.e. non oral) including barrier contraception, long-acting reversible contraception such as such as hormonal implants, hormonal IUDs or copper IUDs - Advise people to use effective contraception to avoid getting pregnant for 12–18 months post-surgery for infant health |
Abbreviations: DEXA, dual-energy x-ray absorptiometry; IUD, intrauterine device; PTH, parathyroid hormone.
Summary of the evidence
- Evidence from several small RCTs, supported by large observational studies, demonstrates that bariatric surgery is an effective long‑term intervention for severe obesity, typically achieving approximately 25–30% total body weight loss in the first year.249,306,341-343
- Several meta-analyses (of predominantly cohort studies) have shown that metabolic bariatric surgery confers significant improvement in cardiovascular risk factors including blood pressure, glycaemia, lipids and waist circumference, compared with medical management.204-206
- Significant reductions in major adverse cardiovascular events of 40–60% have been demonstrated post-bariatric surgery in observational studies. A large meta-analysis of 40 matched cohort studies found that bariatric surgery was associated with a statistically significant reduction in major adverse cardiovascular events, atrial fibrillation, heart failure, myocardial infarction and stroke.197
- A systematic review and meta-analysis of people with established heart failure who underwent metabolic bariatric surgery were found to have a 72% reduced risk of heart failure exacerbations (RR 0.28; 95% CI 0.13–0.55) compared with those with heart failure who had non-surgical treatment.203
- Observational cohort studies provide inconsistent evidence regarding the reduction in atrial fibrillation incidence following metabolic bariatric surgery.187,344
Resources and further reading
- National Association of Clinical Obesity Services. Find a service
- RACGP. Bariatric–metabolic surgery: A guide for the primary care physician
- Healthdirect. Guide to bariatric surgery. 2024. (For consumers)
- Better Health Channel. Obesity surgery. 2022. (For consumers)
- Australian Journal of General Practice. Bariatric surgery. 2025
- Australia and New Zealand Metabolic and Obesity Surgery Society. Public bariatric surgery – A national framework. 2020
- American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for metabolic and bariatric surgery. Surgery for obesity and related diseases. 2022
2. Behaviour modifications
Management algorithm