Australian clinical guideline for diagnosing and managing acute coronary syndromes 2025

Overview
Introduction
This guideline is provided to assist clinicians in the diagnosis and management of people presenting with symptoms suggestive of acute coronary syndromes (ACS), or with confirmed ACS. ACS includes acute myocardial infarction (AMI) and unstable angina (UA), resulting from inadequate blood flow to heart muscle. ACS is a leading cause of morbidity and mortality and is a time-critical medical emergency.
The recommendations are based on contemporary evidence. They should complement, not replace, clinical judgement. Shared decision-making among clinicians, presenting individuals and their families is required and should be based on individual values, preferences and circumstances. Clear communication with individuals and those who support them is critical to these discussions.
This guideline was developed in consultation with a broad range of organisations, clinical experts and people with lived experience, representing different geographic regions, sex, genders, ethnicities, clinical settings and perspectives.
Purpose
This guideline replaces the National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016.
The guideline includes:
- recommendations for assessing and managing people with suspected or confirmed ACS
- a short summary and reference to the available evidence supporting the recommendations
- practical advice on how to apply the recommendations
- specific practice points for assessing and managing ACS in underserved populations.
Scope
This guideline addresses:
- assessment of adults (>18 years) with suspected ACS
- management of confirmed ACS
- recovery after ACS and secondary prevention of future vascular events.
The guideline primarily addresses the management of myocardial infarction (MI) caused by atherosclerotic plaque rupture, ulceration, fissure or erosion. Some recommendations may also apply to other MI types, such as MI due to oxygen supply/demand mismatch without acute coronary occlusion, particularly for acute treatment and post-hospital care (Figure 2). Specific guidance is included for MI due to non-atherosclerotic causes, such as spontaneous coronary artery dissection (SCAD).

Non-acute coronary syndrome presentations, non-cardiac chest pain and related cardiac conditions (e.g. heart failure, risk factors or comorbidities like cancer or diabetes) are outside the guideline's scope. Healthcare professionals should consult existing resources for comprehensive management of these conditions.
Intended audience
This guideline is intended for all healthcare professionals involved in the care of people with ACS, including cardiologists, emergency physicians, paramedics, general practitioners, nurses, nurse practitioners, First Nations health workers and practitioners, pharmacists and other allied healthcare professionals. Although the term ‘general practitioner’ is used throughout, the Heart Foundation recognises that in some communities, other primary healthcare professionals – such as primary care nurses, nurse practitioners, and First Nations health workers and practitioners – are the first point of contact with the health system.
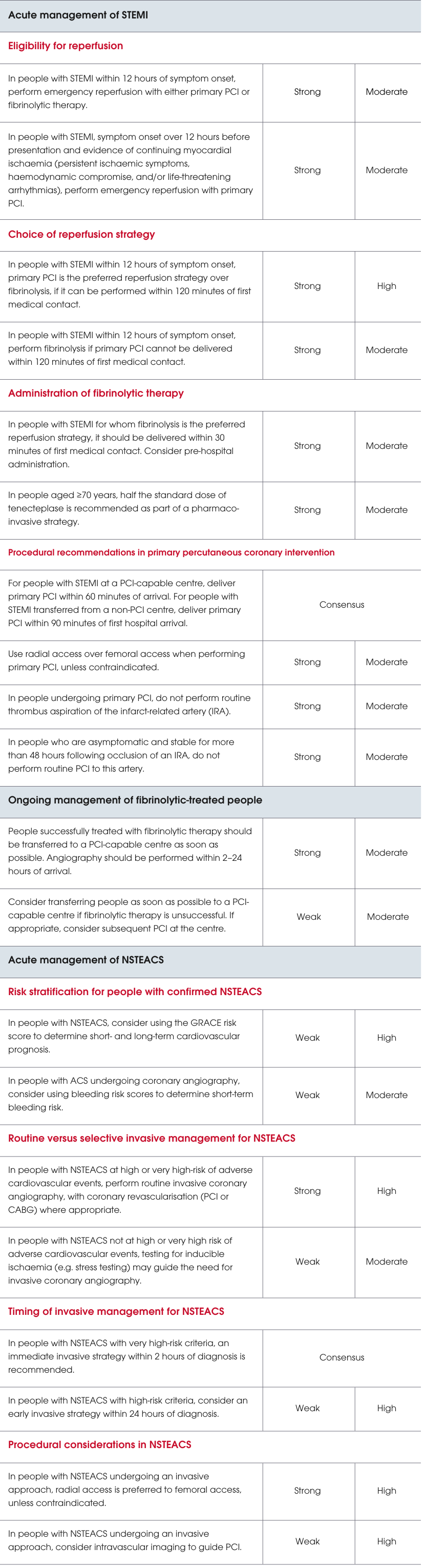
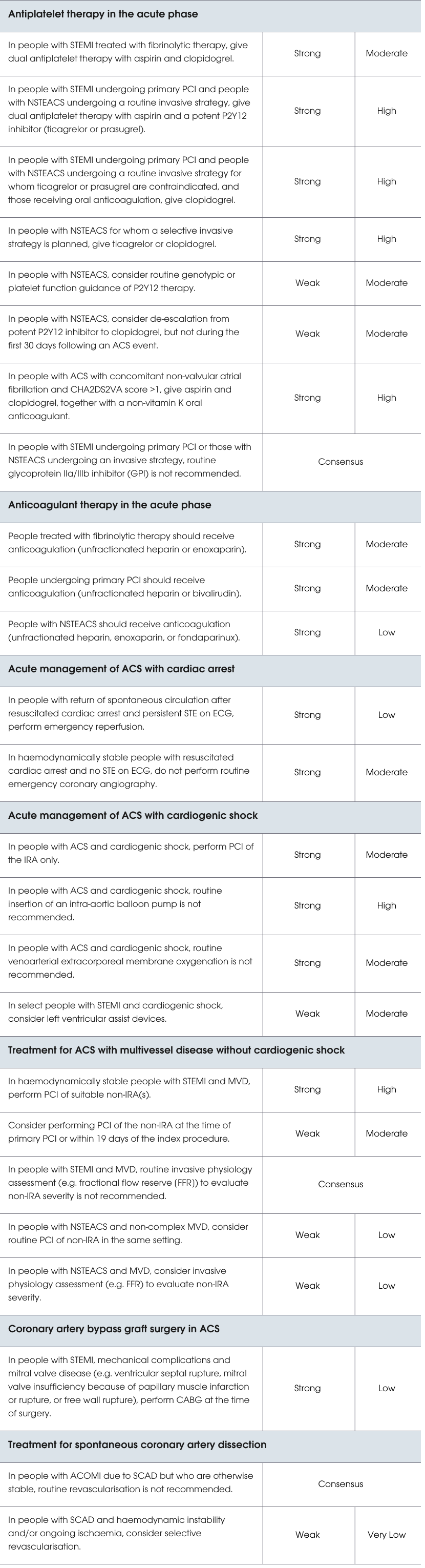
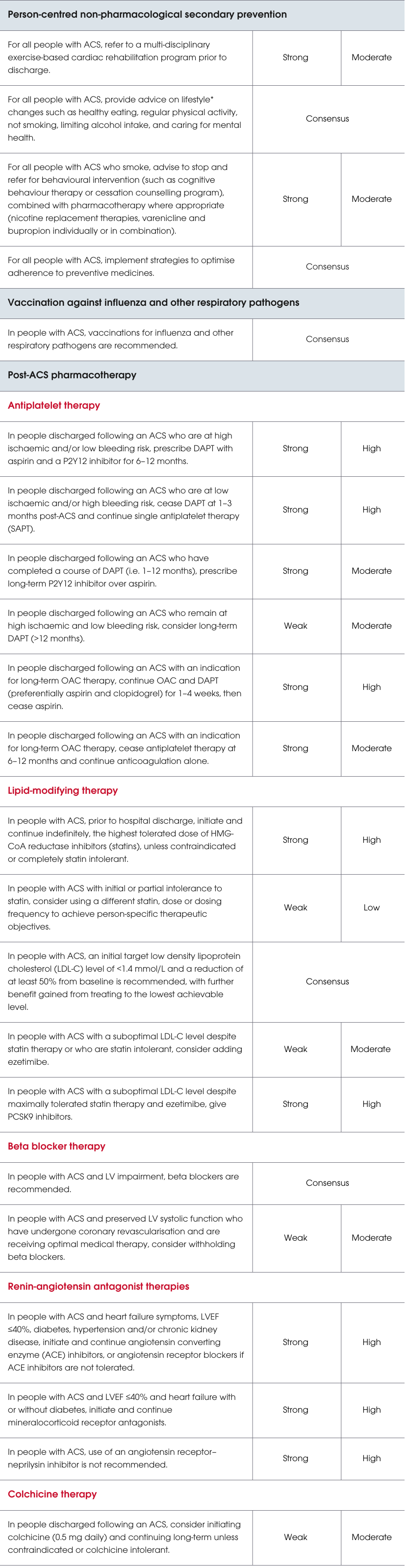
Summary of recommendations
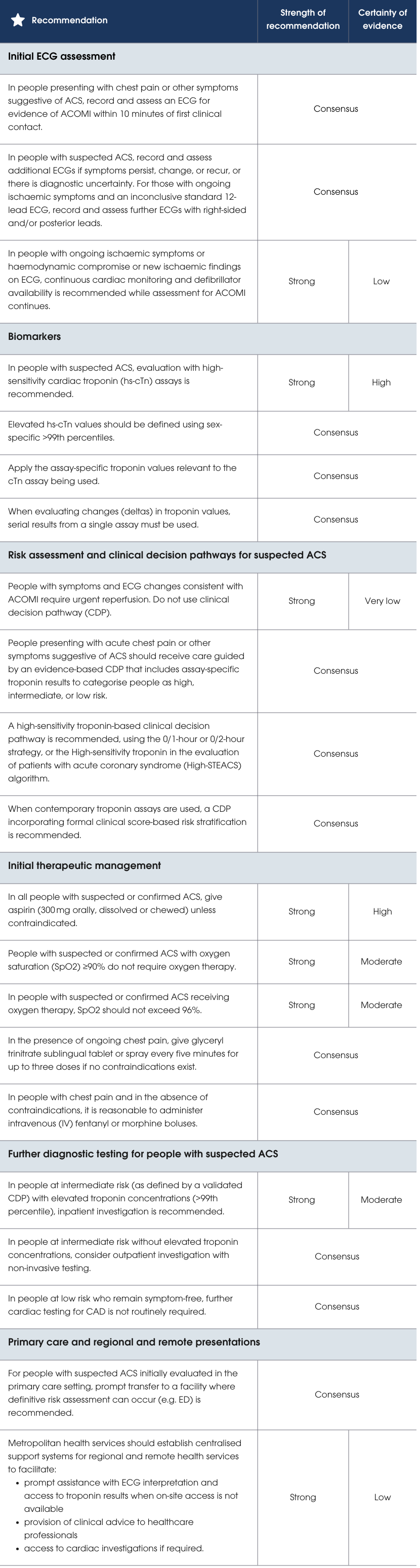
Note: #These recommendations apply to people with ECG changes that may not be recognised as STEMI but are indicative of ACOMI, specifically: high lateral myocardial infarction (MI), posterior MI, right ventricular MI, De Winter T waves, left bundle branch block with modified Sgarbossa criteria.
*Use of the word lifestyle here refers to a collective group of modifiable risk factors. The authors wish to acknowledge that these risk factors are not solely dependent on individual choice, and instead reflect the cultural, social and environmental factors that influence behaviour. This term does not in any way attribute blame to individuals.
Preamble